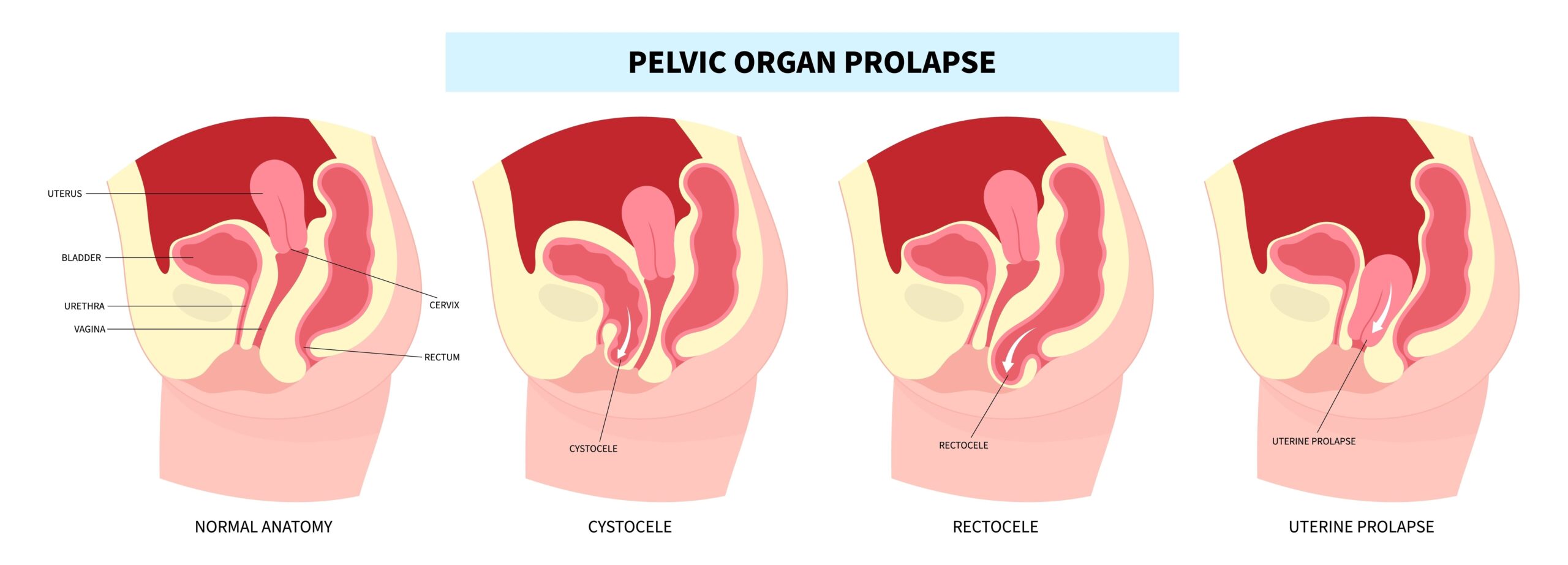
Let’s start with what is a prolapse?
A vaginal prolapse might also be called a pelvic organ prolapse (POP) or in more medical terms a cystocoele, uterocoele or rectocoele. A prolapse is where one or more of the pelvic organs (bladder, uterus or bowel) drops lower down in the pelvis and creates a bulge into the vaginal space. Most commonly women describe the feeling as “something is coming down into my vagina that feels like a lump or a bulge”. This can give women quite a fright if they notice it when they are wiping that area when they are in the shower for example.
Other symptoms might be:
- Difficulty retaining a tampon
- Incomplete emptying of the bladder or bowel
- Symptoms may be worse at the end of the day, following exercise or heavy lifting or straining to empty the bowels
A dragging feeling in the low abdomen or low back
How common is a prolapse?
This is an interesting question. If examined by a doctor or other pelvic health professional, around 50% of women who have ever had a baby (and some who haven’t) would be diagnosed with a prolapse as some degree of bulge could be seen on a vaginal examination. However, only 20% of these women are sufficiently bothered by the symptoms to seek treatment. So, rather than focussing on the anatomical appearance of a prolapse, we focus on how much it is bothering the woman with her general activity and impacting her bladder and bowel function.
Even more interesting is that once there is a mild degree of prolapse it does not mean there will be a “slippery slope” to the prolapse worsening or dropping lower as you age. It can be very dependent on what occurs through menopause – sometimes it is actually better after menopause.
Why does a prolapse happen?
A prolapse occurs due to stretching or tearing of the fascia and ligaments that hold the organs in place. Factors that can contribute to this are pregnancy, vaginal deliveries (particularly with forceps), advancing age, obesity and potentially chronic constipation and heavy occupations. There may be a genetic predisposition.
If I think I have a prolapse, what should I do?
Firstly, visit your GP so that they can conduct an examination and confirm if you do have a prolapse. They may suggest some tests to check for any other causes for your symptoms. Depending on your age and their findings, they may suggest vaginal oestrogen ointment. The next step may depend on the level or stage of prolapse ie how low it is sitting. Basically if it is at the level of the vaginal entrance or higher, the first step will be to see a women’s health physio. If the prolapse is lower than that, the GP will likely refer you to a gynaecologist.
In terms of physiotherapy, your physio will identify any “lifestyle factors” that you could modify. Of vital importance is reducing any constipation as straining to empty your bowels can exacerbate the position of the prolapse as well as how it feels. Your physio can help you with this reducing constipation and teach you how to empty your bowels without straining.
Pelvic floor exercises – improving the strength and function of your pelvic floor muscles can reduce the bother of a mild to moderate prolapse by in around 50% of women.
At Total Physiotherapy we have four expert women’s health and the pelvic floor physiotherapists who are passionate about treating women with conditions such as prolapse.
Pessary – a pessary is a device that is inserted vaginally to support the prolapse. If fitted well you should not be aware of the pessary and the prolapse should be significantly less noticeable when it is in place. For some women, the physiotherapist can fit the pessary and instruct them on how to insert and remove it for when it is needed. For other women a pessary will be best fitted by a gynaecologist. There is now some evidence that rather than just supporting the prolapse while it is in place, the use of a pessary for some women can actually improve the anatomical position.
Surgery – should physiotherapy and other conservative management not provide sufficient improvement in symptoms, surgery is an option that can be discussed with a gynaecologist. In recent years, women have been very concerned about the surgical options because of the problems that occurred when mesh was used for prolapse repair. Rest assured that mesh for that type of surgery is no longer allowed in Australia so it will be not offered to you. There are other surgical options that can be effective. The specialist may recommend pelvic floor physiotherapy following your surgery to optimise your pelvic floor muscles strength.
By Louise Henderson
APA Titled Physiotherapist (Continence and Women’s Health)


